

By Julie Grassian
Problem Statement:
1 in 20 children in the United States experience the loss of one parent or guardian before the age of 15.1 Even more shocking is that 2 million children in the United States have lost both parents before the age of 18.1 Parental death is considered to be among the most difficult of adverse childhood experiences. Childhood is a critical period for development; parents are a crucial source of buffering, supportive relationships against stress, and can promote resilience in the face of adversity.2 Children without parents are at a disadvantage in recovering from stressful situations and regulating their emotions. Experiencing these traumatic events with an absence of supportive, buffering relationships and environments can produce toxic stress, which is prolonged activation of stress response systems as a result of severe adversity.3 This prolonged activation has been linked to the eventual development of depressive disorders.4
Studies have shown that children who experience the loss of a parent or guardian are at increased risk for developing psychological and behavioral health issues, including depression, anxiety, post-traumatic stress disorder (PTSD).5 Studies of adult mental disorders frequently reveal childhood bereavement, suggesting that such loss contributes to the development of these mental health disorders.6 An American Psychological Association study showed that depression was more common for bereaved children, specifically within the first 2 years of loss, than in non-bereaved children.7 Children and adolescents are more likely to experience complicated grief reactions if their grief is not properly addressed early on, leading to increased risk for depression and functional impairments.8 40% of children experiencing grief meet the criteria for major depression one month after their loss, and 24% still meet the criteria after two months.9
During April 2020 to June 2021 alone, more than 140,000 youth experienced the loss of a parent or guardian. Among youth who lost a parent or guardian to a COVID-related death, 65% were children of racial/ethnic minorities.10 In California, racial/ethnic minority youth also experience mental illness at rates above the State average11, and are more likely to have unmet mental health needs compared with their non-Latinx white counterparts.12 These youth are also more likely to attend underfunded public schools that lack quality mental health services.13 This means that communities with the largest percentage of youth impacted by parental loss are the least likely to have adequate resources to address bereaved youth’s needs. It is reported that one in six youth experience a mental health disorder14, specifically depression or anxiety, yet less than 40% of youth are able to access needed mental health services.12 Over the past year, it was reported that 54% of youth struggled to find grief resources.15 Having access to mental health and grief-tailored services is extremely important during childhood. For children that do not have parents, it is crucial that they have access to supportive services to prevent adverse mental health challenges that may accompany their grief.
Policy Alternatives:
Policy Recommendation 1: Grief-Focused Mental Health Services in Public Schools
It is crucial that youth impacted by parental loss have access to grief-informed care. Schools can be a perfect place to integrate grief focused mental health interventions as this is where youth spend the majority of their awake hours. Yet, we still fail to provide adequate mental health services in schools. Prior to COVID-19, 7 in 10 teachers had at least one student in their class who had lost a parent or guardian.1 It has been shown that untreated mental health issues impact student attendance, behavior, and readiness to learn.16 The Mental Health Services Act (MHSA) was enacted in 2004, with the goal of improving the public mental health system in California by providing early intervention and treatment.17 However, we have yet to see sufficient mental health services inside school settings that are effective and long-term. The current mental health services offered in school-based settings are brief interventions focused on academic counseling and behavioral issues.17 These services need to be improved to provide long-term, quality, grief-focused mental health support. Schools can play a leading role in the prevention and treatment of student mental health needs related to grief and parental loss. Schools offer regular and consistent supportive relationships for youth, which is extremely important for youth without parents who would otherwise not have access to these relationships. For many youth, schools are the only place where they can access mental health services, and youth are more likely to seek out mental health services when they are offered in schools.18
Policy Recommendation 2: Partnering with Existing Grief-Focused Mental Health Services
There are insufficient grief-specific services offered specifically in school settings, however there are grief services available through community organizations and nonprofits that schools can partner with. California School-Based Health Alliance is a statewide nonprofit that promotes trauma-informed mental health services in schools by integrating these services into schools that serve predominantly low-income students of color, who are less likely to have access to mental health services.19 In April 2020, Alameda School District recently partnered with Care Solace to connect youth with community-based mental healthcare resources and providers.20 Additionally, Children’s Hospital Los Angeles National Center for School Crisis and Bereavement provides an interdisciplinary team of medical, mental health, and school professionals that assist with grief services for schools and communities.21 School partnerships with existing mental health services have been shown to increase high school graduate rates and improve the academic success of students.22 Partnering with outside organizations such as these are a first-step in effectively integrating grief focused mental health services into schools. However, we need to take this a step further and fully integrate these services to be permanently offered in school settings.
Policy Recommendation:
It is imperative that comprehensive, culturally responsive grief focused mental health services are accessible in public schools. Grief counselors and childhood mental health specialists need to be integrated into school-based settings so that they are easy to access for youth who need it most. By doing this, screenings and assessments can be conducted early, treatment can be provided, and specialists can connect students to more intensive services in the community if needed. This will also help to reduce the stigma associated with mental health and grief when these services are normalized in school settings.
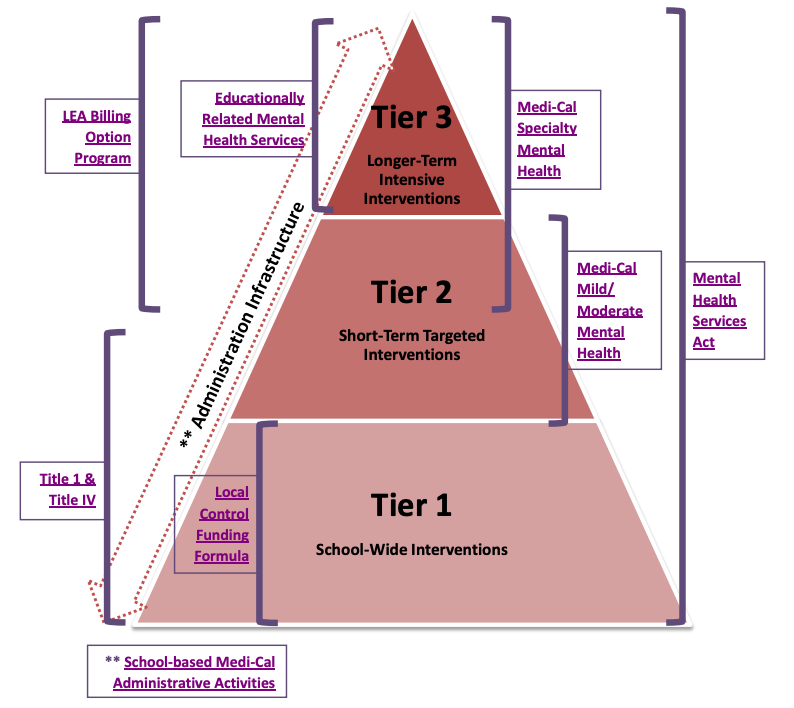
Integrating comprehensive, grief-focused mental health services into public schools can be a reality for our youth. In California specifically, the funding is available, it just needs to be properly utilized. There are three main tiers of interventions, and there are funding streams available for each intervention tier.24 It is essential that funding from all three tiers are utilized. Tier 1 are school-wide interventions, tier 2 are short-term targeted interventions, and tier 3 are longer-term intensive interventions. Among tier 1, a funding stream available includes School-Based Medi-Cal Administrative Activities. This would give schools the option of becoming a contracted provider of speciality mental health services, or to contract with community mental and behavioral health agencies. Title 1 & Title IV provides federal funding for both tier 1 and tier 2 interventions through the Every Student Succeeds Act (ESSA), particularly for schools that serve low-income populations. This funding can be utilized for schools to fund mental health providers, support provider training, and establish partnerships with grief-focused community organizations. Additionally, to address tier 3 interventions, funding through Educationally-Related Mental Health Services (ERMHS) is available. ERMHS offer funding for various mental health services to support children with disabilities with access to mental health services, including individual counseling, social work services, and psychological services.
By utilizing the various funding streams available, schools can successfully and permanently incorporate grief-focused mental health services. This funding can contract grief counselors, social workers, and other grief-focused mental health specialists, who are essential to address the needs of bereaved youth who have experienced parental loss. Especially given the COVID-19 pandemic, grief and loss are a pressing issue and schools must properly provide support for youth experiencing loss. We can see a world where our youth receive quality mental health support in schools, are able to connect with other students with similar experiences, and where mental health is destigmatized among students. We can change the mental health trajectories of youth who have experienced loss. Grief can result in resiliency, if given sufficient resources and attention. Youth’s grief deserves to be tended to, and it’s time we give these children the support they deserve.
References
1. Children and Grief Statistics. (n.d.). 2. https://www.childrensgriefawarenessday.org/cgad2/pdf/griefstatistics.pdf
2. Resilience. (n.d.). Center on the Developing Child at Harvard University. Retrieved December 5, 2021, from https://developingchild.harvard.edu/science/key-concepts/resilience/
3. Toxic Stress. (n.d.). Center on the Developing Child at Harvard University. Retrieved October 19, 2021, from https://developingchild.harvard.edu/science/key-concepts/toxic-stress/
4. Heim, C., Newport, D. J., Mletzko, T., Miller, A. H., & Nemeroff, C. B. (2008). The link between childhood trauma and depression: Insights from HPA axis studies in humans. Psychoneuroendocrinology, 33(6), 693–710. https://doi.org/10.1016/j.psyneuen.2008.03.008
5. Bergman, A.-S., Axberg, U., & Hanson, E. (2017). When a parent dies – a systematic review of the effects of support programs for parentally bereaved children and their caregivers. BMC Palliative Care, 16(1), 39. https://doi.org/10.1186/s12904-017-0223-y
6. Osterweis, M., Solomon, F., & Green, M. (1984). Bereavement During Childhood and Adolescence. In Bereavement: Reactions, Consequences, and Care. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK217849/
7. Brent, D., Melhem, N., Donohoe, M. B., & Walker, M. (2009). The Incidence and Course of Depression in Bereaved Youth 21 Months After the Loss of a Parent to Suicide, Accident, or Sudden Natural Death. American Journal of Psychiatry, 166(7), 786–794. https://doi.org/10.1176/appi.ajp.2009.08081244
8. Slomski, A. (2021). Thousands of US Youths Cope With the Trauma of Losing Parents to COVID-19. JAMA, 326(21), 2117–2119. https://doi.org/10.1001/jama.2021.20846
9. Grief By The Numbers: Facts and Statistics. (n.d.). The Recovery Village Drug and Alcohol Rehab. Retrieved December 5, 2021, from https://www.therecoveryvillage.com/mental-health/grief/related/grief-statistics/
10. More than 140,000 U.S. children lost a primary or secondary caregiver due to the COVID-19 pandemic | National Institutes of Health (NIH). (n.d.). Retrieved December 6, 2021, from https://www.nih.gov/news-events/news-releases/more-140000-us-children-lost-primary-or-secondary-caregiver-due-covid-19-pandemic
11. Existing Disparities in California’s System of Specialty Mental Health Care. California Pan-Ethnic Health Network, 30 July 2019, from https://cpehn.org/about-us/blog/existing-disparities-in-californias-system-of-specialty-mental-health-care/#_ftn1
12. American Psychological Association, Working Group for Addressing Racial and Ethnic Disparities in Youth Mental Health. (2017). Addressing the mental health needs of racial and ethnic minority youth: A guide for practitioners. Retrieved from www.apa.org/pi/families/resources/mental-healthneeds.pdf
13. Adrienne Y. StithClyde H. Evans & Brian D. Smedle. (2001). The Right Thing to Do, The Smart Thing to Do: Enhancing Diversity in the Health Professions: Summary of the Symposium on Diversity in Health Professions in Honor of Herbert WNickens, MD. National Academies Press. Retrieved from https://www.nap.edu/catalog/10186/the-right-thing-to-do-the-smart-thing-to-do
14. Mental Health in Schools | NAMI: National Alliance on Mental Illness. (n.d.). Retrieved December 6, 2021, from https://www.nami.org/Advocacy/Policy-Priorities/Improving-Health/Mental-Health-in-Schools
15. Childhood Grief Facts & Figures—Experience Camps. (n.d.). Retrieved December 5, 2021, from https://experiencecamps.org/childhood-grief-facts-and-statistics
16. Barrett, S., Eber, L., & Weist, M. (2013). Interconnecting School Mental Health and School-Wide PBIS. 2, 137.
17. Mental Health Services Program Overview—Mental Health (CA Dept of Education). (n.d.). Retrieved December 5, 2021, from https://www.cde.ca.gov/ls/cg/mh/mentalhealth.asp
18. Resources & Podcasts. National Association of School Psychologists (NASP). (n.d.). Retrieved December 6, 2021, from https://www.nasponline.org/resources-and-publications/resources-and-podcasts
19. Locations | California School-Based Health Alliance. (2011, October 26). https://www.schoolhealthcenters.org/school-based-health/locations/
20. Mental Health Resources. (n.d.). Retrieved December 5, 2021, from https://www.alameda.k12.ca.us/mentalhealth
21. About Us. (2020, June 24). National Center for School Crisis and Bereavement. Retrieved December 5, 2021, from https://www.schoolcrisiscenter.org/about/
22. “National Council for Mental Wellbeing – Homepage.” National Council, 18 Aug. 2021, https://www.thenationalcouncil.org/
24. Public Funding for School-Based Mental Health Programs – California courts. (n.d.). Retrieved December 6, 2021, from https://www.courts.ca.gov/documents/BTB25-MHReform-08.pdf
Julie (she/her) is a Master of Public Health and Master of Social Welfare student at UC Berkeley. She is passionate about addressing childhood loss/adversity and its effects on mental health outcomes. Her career goals are to improve access to mental health services in public schools and provide grief-informed care to underrepresented youth.
The views expressed in this article do not necessarily represent those of the Berkeley Public Policy Journal, the Goldman School of Public Policy, or UC Berkeley.